
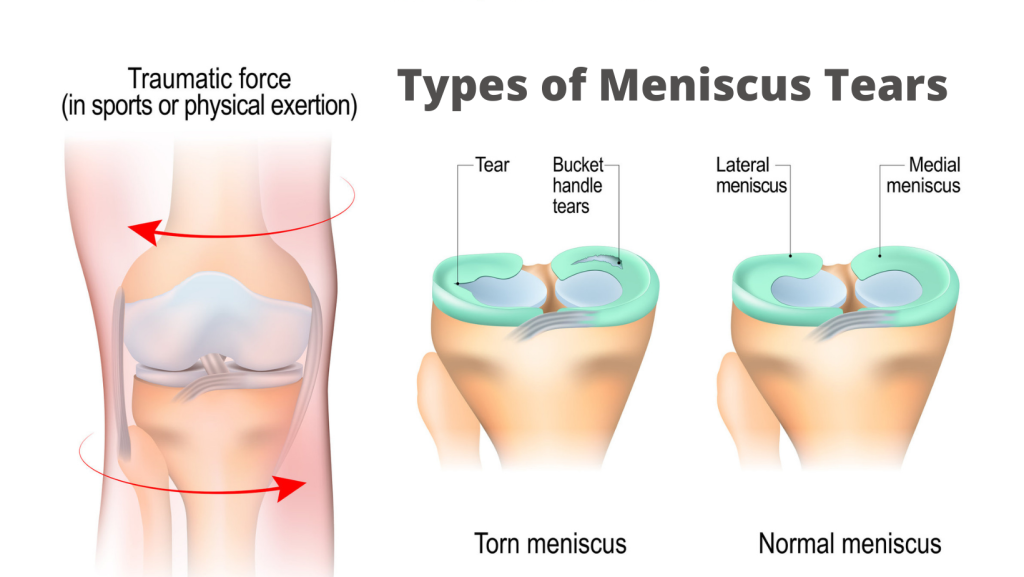
This weekend, I am in New York City seeing a couple of patients and visiting with my two sons, who now live in the East Village. About 10 weeks ago, my 20-yo was goofing around with his girlfriend (getting a piggy back ride) although he weighs twice as much as her. He fell on a twisted foot and immediately experienced knee pain that was severe, limiting his ability to flex the knee. There was mild clicking and the pain was worsened while twisting on the single leg. There is only one thing this could be: a torn meniscus.


1 thought on “Torn joint cartilage”
fantastic! timing is everything