

My previous three blogs about the public health context, the apocalyptic death cult, and the exaggeration of the threat have been my attempts to contextualize what is happening.
This fourth blog is an attempt to explain what we know about coronaviruses generally and about this strain particularly. Read until the end to be rewarded with some really good news for a change.
First off, any virus is not alive in the sense that it cannot exist without a host cell. We can use the borrowed term from computer science to explain: a computer virus is a clever set of instructions that cannot exist without a computer. In the case of this coronavirus, it is a 125nm sphere with club like Spike proteins that bind to angiotensin-2 receptors to enter the cells of the respiratory system.
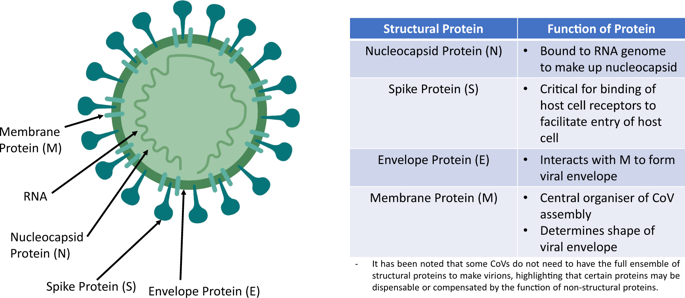
The actual structure of the coronavirus is quite easy to visualize in this cartoon and you will see again in the gene maps below. The major structural components are comprised of the Spike protein (S), membrane (M) and envelope (E) proteins, as well as the the nucleocapsid proteins (N) that bind the coding RNA. The RNA is the complete blueprint for producing all the required proteins of the virion (or viral particle). It is called “corona” because the spoke proteins give it a halo, or fuzzy crowed appearance under electron microscopy.
Once inside a cell, the positive sense (meaning coding for proteins) finds its way to the host cells manufacturing plant, known as the endoplasmic reticulum, The RNA message hijacks the normal mechanisms for protein synthesis to make its own proteins including its own replicase (the RNA copying machine). By some magic we don’t fully comprehend the host machinery and its own replicase manages to reproduce all the components of the future viruses and they are packaged into many copies of the virion (or viral package) which are released by the host cell into the bloodstream. This process inhibits clinically inhibits host immunity, triggers cytokine inflammatory storm, and doesn’t usually explode the host cell in the process (lysis).
You may want to read this excellent review article from 2016 by Fehr and Perlman. They review the phylogeny of Coronviruses, structural and biochemical considerations, epidemiology, and clinical implications in some detail. Here is an excerpt:
Prior to the SARS-CoV outbreak, coronaviruses were only thought to cause mild, self-limiting respiratory infections in humans. β-coronaviruses HCoV-229E and HCoV-OC43 were isolated nearly 50 years ago.These viruses are endemic in the human populations, causing 15–30% of respiratory tract infections each year. In most cases of self-limited infection, diagnosis of coronaviruses is unnecessary, as the disease will naturally run its course.
Yes, I know many have been convinced by group think that this situation is different and we will address that later but the implications of what the authors say are important enough to restate. ENDEMIC means coronaviruses are always in the human population (for at least 50 years) and comprise 15-30% of annual cold infections. This means if there is lasting serology (antibodies) specific to coronavirus, the hysteria will only be magnified because we have all had colds and suddenly we will consider ourselves to be lepers rather than someone who had the common cold in the past. Most people get 2-3 colds per year and although most of those were the Rhinovirus, many of them could have been coronavirus.
In this study of coronavirus antibody cross reactivity, researchers found that healthy donors were carrying evidence of old coronavirus infection (229E and OC43) so the devil of antibody testing will be in the details. Can you imagine testing people with a non-specific antibody test and having to explain it to the general public? Here is a quote from that 2005 paper:
Results were positive for IgG antibodies by IFA in 98% (HCoV-229E), 100% (HCoV-OC43), and 1% (SARS-CoV) of the serum samples from healthy donors
In other words, you and I would show evidence of remote infection with this common cold virus 98% of the time for 229E, 100% of the time for OC43, and even the potentially deadly 2003 SARS-CoV 1% of the time. Until we are sure of the specificity of antibody testing to this “novel” bat SARS-CoV2, we need to be careful to not use serology. Instead, we have to reply on PCR tests that are specific for this strain of coronavirus (fingers crossed that they are choosing the correct sequences).
Now, we need to get a little deeper into the weeds as to how “Novel” this strain is. Again, from the Fehr and Perlman paper, we get this helpful image comparing some of these coronavirus of the same family:
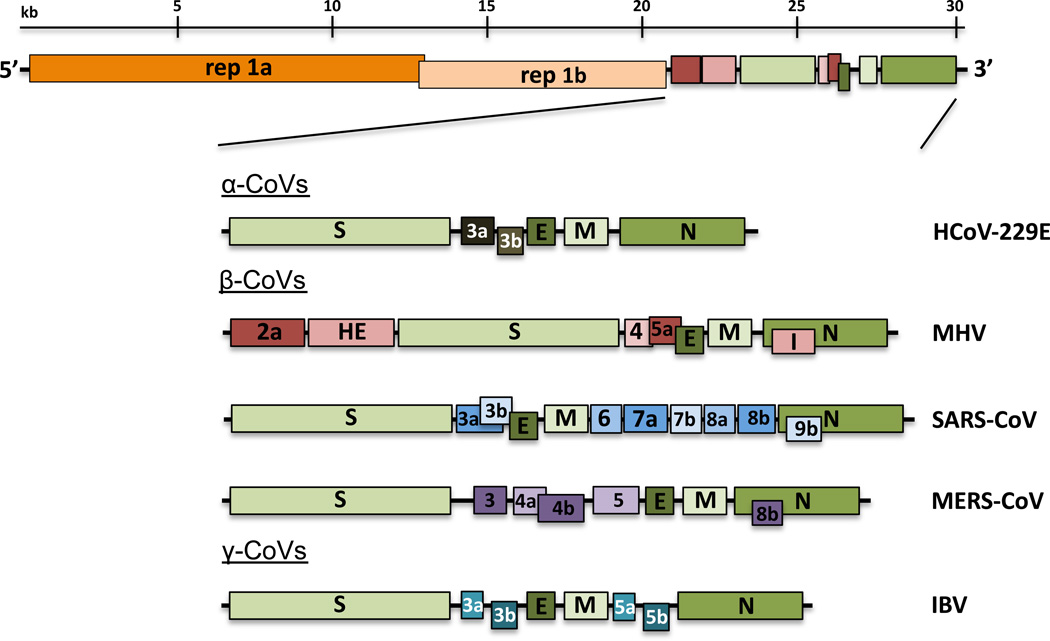
This is the whole virus RNA genome. The orange and peach regions are 20 of 30 thousand base pair regions of the genome that code for the replicase (RNA producing) enzymes. The question of how “novel” lies mainly in the differences in the right side of the genome which encode the other structural and non-structural proteins.
It is important to note the authors point out that both alpha and beta Coronoviruses have been endemic to humanity for over 50 years. Some people have attempted to tie the Gates foundation to the coronavirus, but the patent filed by the Pirbright Institute in 2015 does not suggest they bio-engineered a new coronavirus. Here is a useful phylogeny of all the known coronaviruses from that patent filing.
- Alpha
- Canine coronavirus (CCoV)
- Feline coronavirus (FeCoV)
- Human coronavirus 229E (HCoV-229E) [“common cold” 98% prevalence]
- Porcine epidemic diarrhoea virus (PEDV)
- Transmissible gastroenteritis virus (TGEV)
- Human Coronavirus NL63 (NL or New Haven)
- Beta
- Bovine coronavirus (BCoV)
- Canine respiratory coronavirus (CRCoV)—Common in SE Asia and Micronesia
- Human coronavirus OC43 (HCoV-OC43) [“common cold” 100% prevalence]
- Mouse hepatitis virus (MHV)
- Porcine haemagglutinating encephalomyelitis virus (HEV)
- Rat coronavirus (Roy). Rat Coronavirus is quite prevalent in Eastern Australia where, as of March/April 2008, it has been found among native and feral rodent colonies.
- (No common name as of yet) (HCoV-HKU1)
- Severe acute respiratory syndrome coronavirus (SARS-CoV) in 2003
- Middle East respiratory syndrome coronavirus (MERS-CoV)
- Gamma
- Infectious bronchitis virus (IBV) [the subject of the their patent and the Israeli vaccine below]
- Turkey coronavirus (Bluecomb disease virus)
- Pheasant coronavirus
- Guinea fowl coronavirus
- Delta
- Bulbul coronavirus (BuCoV)
- Thrush coronavirus (ThCoV)
- Munia coronavirus (MuCoV)
- Porcine coronavirus (PorCov) HKU15
The Covid-19 (for 2019) has unfortunately been called SARS-CoV-2. So the real question is how different is this from SARS-CoV that we already faced in 2003 that killed 349 and infected 5300 in China? In this diagram from Andersen et al, you can read the letters and their order signifying the amino acids coded for in the spike protein. There appears to be a great deal of similarity but this is the detail that you are looking for:
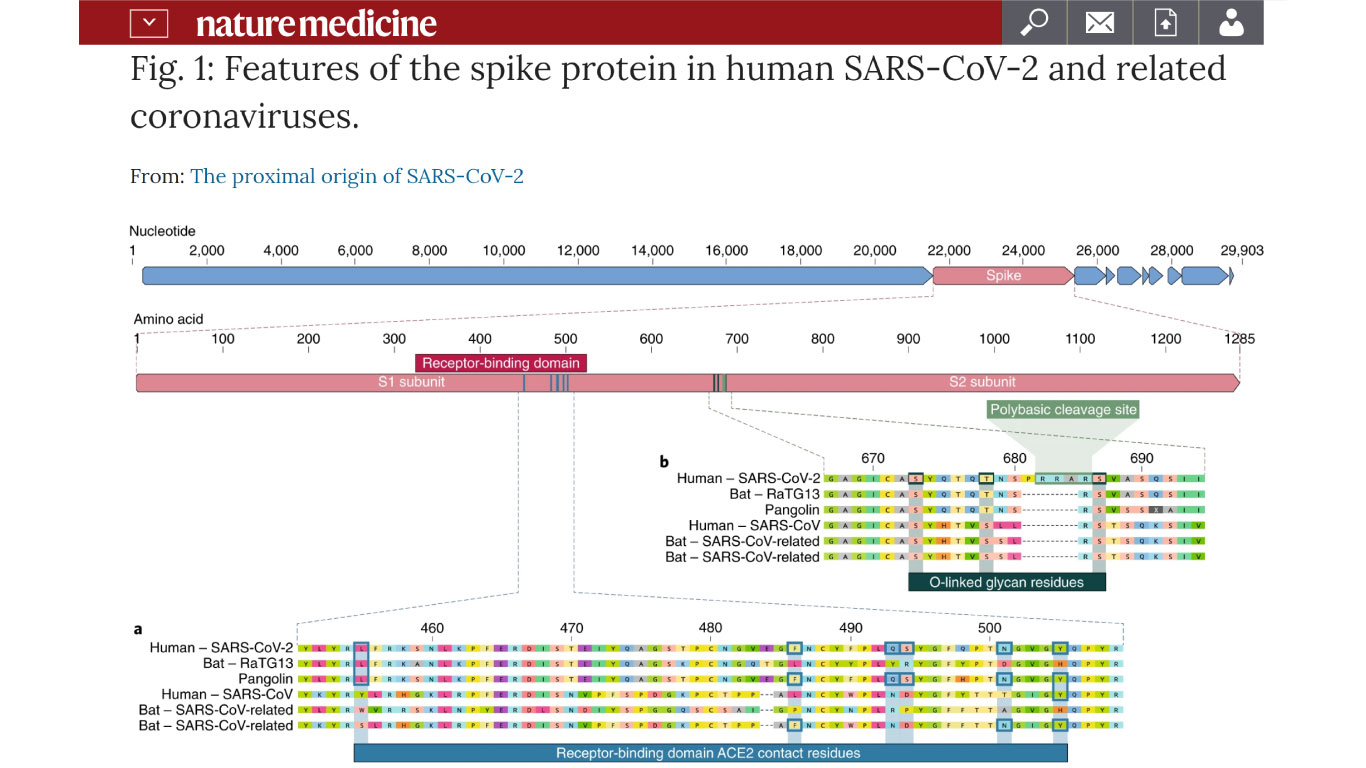
So with regard to this area of the genome, comparing the top line with the 4th line), the viral genome looks very similar. It is impossible to say whether this difference in binding to the angiotensin-2 receptor represented by these changes is significant. If the behavior clinically is different the answer may also lie in the non-structural proteins or any of the other proteins or processing factors in the RNA.
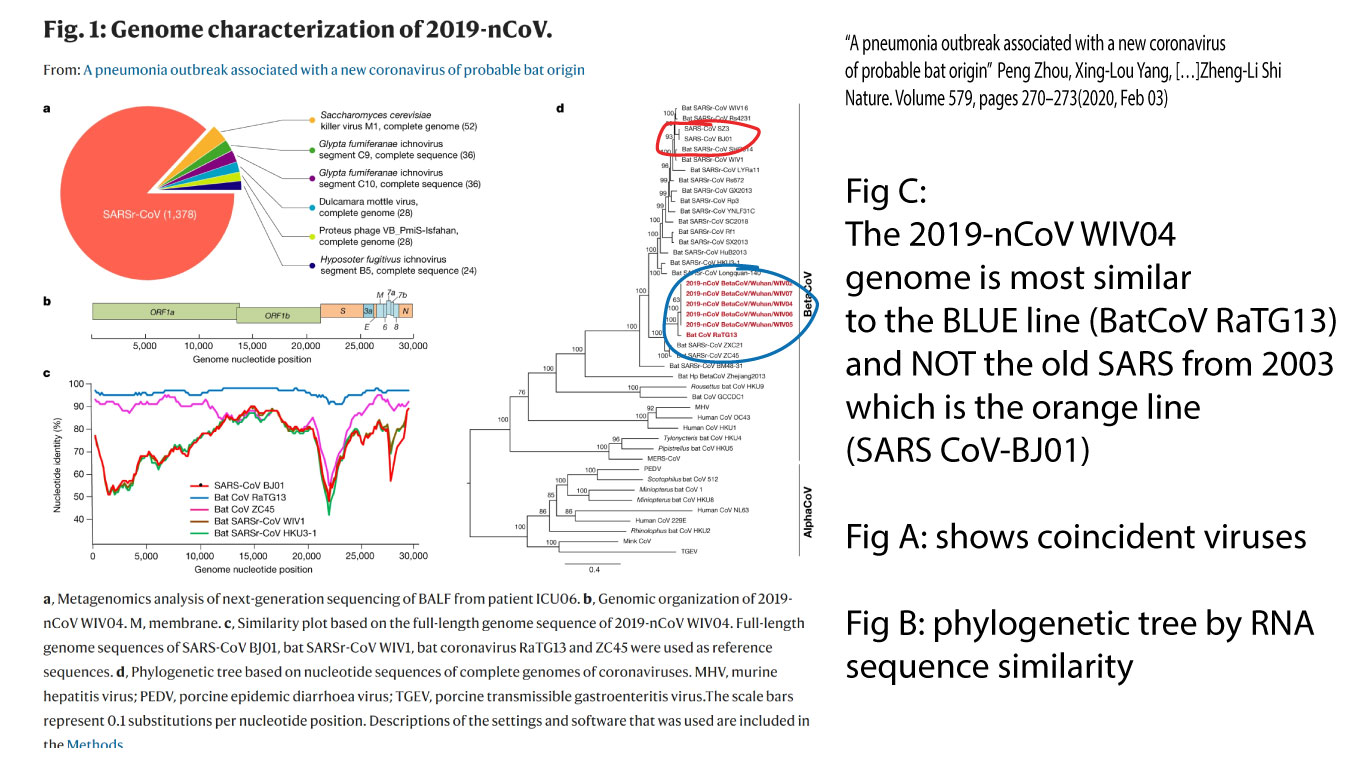
Long-time coronavirus researcher at the Wuhan Insitutue of Virology, Shi Zheng-li, published this paper comparing the SARS-CoV-2 versus other coronaviruses and concluded that because it shares 96% sequence homology with a Bat CV and only 80% homology with the previous SARS-CoV, that it was probably a zoonosis (infection from non-human animal) recombination event. Here is her phylogenetic tree made from inferences from sequence homology:
It is helpful to remember at this point that these viruses are not exclusive to bats OR humans. The origin and prevalence is irrelevant and we know that even our dogs can become infected. In the absence of any evidence to the contrary, it is hard to argue that this was engineered because of the similarity the “novel” virus shows to other beta-coronaviruses that occur in bats and humans. If you want to do a really deep dive as to how that happens, read this article from 2015.
At this point in the blog, most people are probably thinking, “so what? I’m even more confused now that I know a little more.” As I explored in this blog, the wise man encounters this as an aphorism: “the more I know, the less I understand.”
So let us turn to more practical aspects of our current situation since the bottom line is that short of someone coming forward and confessing to making this version, the experts believe that it may be more closely related to the bat version than the previous human version that caused SARS and MERS.
The first real problem is that of testing. Because of contamination, the WHO version of the tests had an estimated 50% false positive rate. That is totally unacceptable and using them would have caused wide-spread hysteria. Currently, only 10% of those with symptoms are testing positive in the US. Secondly, testing serology, or the presence of old antibodies from infection may cross react with fommon versions of the virus making the use of those tests also alarming and clinically irrelevant.
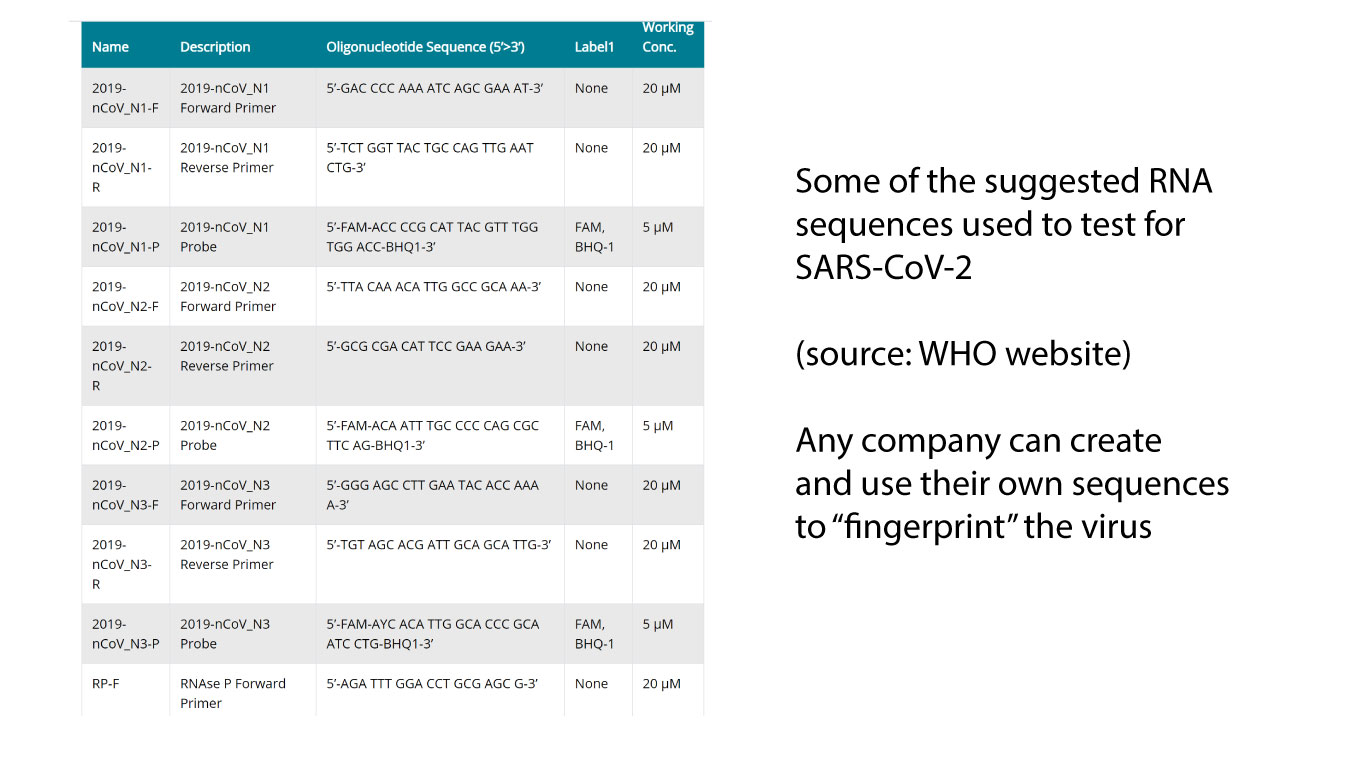
The state of the art is to take a sequence of viral RNA and make a PCR primer that detects it. The WHO website lists twelve sequences that are used to “fingerprint” this virus but no one can say the relative sensitivity, specificity, false-positive, or false-negative rates of them and to what extent they are detecting other versions of coronaviruses.
“Garbage-in, garbage-out” but if the testing kits that are not contaminated like the WHO made then sensitivity and specificity of PCR testing is usually quite high. We don’t know if the sequences they used were specific to this strain but we hope they are good enough at their jobs to take that into account.
If you are hoping for a medical hack, you are in luck as clinicians are reporting decreased disease severity with old drugs (see below). In addition, my colleague Doug Spiel recently improved a severe intubated case of ARDS with use of IV exosomes.
With regard to vaccination, we must be cautious to hang our hopes on that as public health measures and natural immunity may be our best recourse. I will again excerpt from the Fehr and Perlman 2015 review article and put in bold the important concepts along with my commentary.
“Only limited options are available to prevent Coronavirus infections. Vaccines have only been approved for IBV, TGEV, and Canine CoV, but these vaccines are not always used because they are either not very effective, or in some cases have been reported to be involved in the selection of novel pathogenic CoVs via recombination of circulating strains [they encourage newer versions of the virus].
In the case of SARS-CoV, several potential vaccines have been developed but none are yet approved for use. These vaccines include recombinant attenuated viruses, live virus vectors or individual viral proteins expressed from DNA plasmids. In general, it is thought that live attenuated vaccines would be the most efficacious in targeting coronaviruses. [you are given a weakened version of SARS-CoV to trigger natural immunity]. Despite this success, vaccine development for coronaviruses faces many challenges [107]. First, for mucosal infections, natural infection does not prevent subsequent infection, [blood antibodies don’t work well to prevent entry through the airways and GI tract] and so vaccines must either induce better immunity than the original virus or must at least lessen the disease incurred during a secondary infection.
Second, the propensity of the viruses to recombine may pose a problem by rendering the vaccine useless and potentially increasing the evolution and diversity of the virus in the wild [108]. Finally, it has been shown in FIPV that vaccination with S protein leads to enhanced disease [109]. [this was in cats but showed vaccination led to worse disease] Despite this, several strategies are being developed for vaccine development to reduce the likelihood of recombination, for instance by making large deletions in the nsp1 [110] or E proteins [111], rearranging the 3′ end of the genome [112], modifying the TRS sequences [113], or using mutant viruses with abnormally high mutation rates that significantly attenuate the virus [114]. [this is basically creating mutant strains of weakened viruses].”
In the last instance, the idea of creating a Frankenstein coronavirus that would be intentionally introduced is a very reckless game. As the authors suggest, vaccines don’t work well for mucosal infections, a weakened CoV might not replicate well enough to produce a response, and vaccines can create natural selection pressure for further mutation (like with antibiotic resistance.) As counter-intuitive as it may seem, the best course in treating the herd might be in trusting the herd’s immunity because attempts to intentionally introduce an engineered live viral vaccination program are tantamount to playing god.
Why can’t we just have a vaccination to the S spike protein that would attack all coronaviruses? I don’t know but much greater minds than mine haven’t been able to do it but we will see what comes down the pike. Even our wild-type immunity fails to protect us as mentioned above since 80% of those who get the virus have detectable antibodies (see page 535 of this book chapter). If someone suggests a live virus infection, I would have to seriously consider the wisdom of that versus taking my chances with natural infection given my immune competence and unknown unknowns but that is a debate for a future time.
Let’s tackle one final aspect of the current situation: rumors of 5G involvement. 5G is faster but less able to penetrate. This tech is used in airport scanners and because of its short range, it is an enabling technology for the coming IoT (internet of things). Many authorities suggest it is safe and some have attempted to tie its deployment in Wuhan and on the Diamond Princess as a co-factor in virulence. I have no opinion on this but I do find it interesting that Mill Valley (where tech entrepreneurs live, Brussels (where EU officials work), and Israel (where the tech was invented) are not planning on deploying 5G networks.
What is the take home message of this fourth COVID-19 blog? Yes we battle coronaviruses every year but this strain appears to be a recent zoonosis (disease from animals) that has certainly taken a huge economic toll. By the numbers, it is much more serious than the original SARS or MERS outbreaks although the scale is still three orders of magnitude less than influenza. We don’t know what the natural course would have been through world because of the intense focus and preventative measures taken.
Vaccination for this type of disease is not likely to be effective based on previous attempts although perhaps a vaccine based on an spike protein epitope might be coming. To address the problems with vaccination, an Israeli company working on an inhaled substance to stimulate airway immunity to IBV (a coronovirus causes bronchitis in poultry) wants to change the sequence to match the current CoV and bring it to market.
Some reading this blog might think, “so has he changed his mind about Covid-19?” After doing a deeper dive, I have come to the conclusion that this is probably new, from bats, that testing is fraught with risks, and that vaccines may not help although they certainly will be promulgated. In my first blog, I explained about the importance of hand washing. In my second, I explained that this was a death cult. In my third, I explained that aging and loss of immune competence is the real threat. If you think you know a lot about the common cold, consider 15-25% of your annual colds are from the older coronaviruses despite 80% of us having antibodies to them (see page 535).
What’s more interesting is that this study of people sick enough to be admitted to hospital, the “common cold” of CoV229E and OC43 had a 22.7% and 11.6% chance of mortality respectively because of co-infections and co-morbidity (having other medical problems). Sounds a lot like what is going on now with this “novel” strain.
Lies, damned lied, and statistics. If you are admitted to the hospital with the cold and you are not healthy, you have a high chance of dying, even from what started out as the “common cold”. Is this bat derived strain more contagious and deadly? We don’t know. But we know it is killing older, sicker people at total numbers that are 1/1000th less significant than the flu.
Interestingly, because everyone believes this is different, younger people are being hospitalized resulting in aggregate death rates that are lower that the “common cold” cited above. Panic among younger people who would have previously toughed it out at home if they thought is was the “common cold” is what is taking up the hospital beds and exposing more health care workers to the disease. The Italian shortage of ventilators has not happened in the US or elsewhere and is the result of a lot of old people and a scarcity of ventilators.
If you made it this far, you deserve some good news. Although some disbelieved the “stable genius” president when he pitched Chloroquine+Azithromycin for treatment several days ago, there are now three studies (China, Australia, and France) suggesting 100% response within 6 days of therapy.
Humans are resourceful, our immune systems are powerful, and we should be back to normal soon! Hopefully, the coronahysteria won’t result in wholesale loss of civil liberties, forced vaccinations, and a diminution of our ability to pursue happiness. After every flood, however tumultuous, comes a rainbow. Let’s pray the rainbow comes soon.


7 thoughts on “COVID-19: Origins, Detection, and Cures”
Why would the enhancement of the “batty” version to introduce vie through meat consumption to humans esp. since one cite indicated the bat immune response appears superior to human and other mammals as they(bats), like skunks are able to coexist with the rabies virus while we and other mammals seem limited at best when exposed.
These are simply molecular mechanical structures with some type of affinity(probably “pressure” variant) through existing vortex flow with mass reproduction probability resulting in resource procurement in an environment rich in required atomic nutrition.
Whether animal, human, etc. origin and “natural” or premeditated transmutation, what is original coalescence of these viral entities?
https://www.youtube.com/watch?v=J6VEYzwSdZU&list=PLMNj_r5bccUzQU3UD35dPoYBUKCOdI7Sc
Good one. Answered a lot of my questions. Thank you!
How can I forward this to friends.
Great article!
As always, many thanks Dr. Park, for your insights and wonderful work.
Jim
More great insights! I’ll continue to read your blogs as this story unfolds. Thanks Dr. Park!
Pingback: COVID-19: Lies, Damned lies, and Statistics | Recharge Biomedical