
In my first six blogs about COVID-19, I attempted to explain 6 things:
- Public health context of reducing spread: hand washing, fomites, and quarantine
- The emergence of an apocalyptic death cult. People harbor religious beliefs about COVID-19
- The greater scale of aging as a threat and how it contributes to all-cause mortality
- Coronavirus biology: origins, testing, and therapeutics
- How inflammation produces ARDS, the final common pathway for death from flu-like illnesses.
- Epidemic modeling.
This seventh post will attempt to explain how the body protects itself from viruses and how we do testing. These are topics that can be difficult to understand but I will try to make them as simple as possible. We will discuss natural viral immunity, then adaptive immunity with antibodies, and that will lead to a discussion of testing regimens. It is very much within your grasp to understand everything in this blog, especially if you avail yourself of the helpful videos.
A recurring theme of science in general and this situation in particular is that no one has definitive answers. The first question is how long the virus lives and how it is spread; there is a great deal of controversy. Let’s just say that all viruses can be killed with solvents like soap and alcohol and that covering the eyes and lower face as well as avoiding touching those areas is a good practice. It appears that there is transmission via feces as well so wash your hands well and use a towel to use door handles and bathroom fixtures.
The first physical means of defense from viruses involves the filtering of particles by the nasal hairs and the presence of fluids such as tears, mucous, and phlegm that can suspend and wash away particles. You can drink small amounts of warm water frequently to wash viruses into the acidic stomach and gargle with mouthwash (or strong liquor) to sterilize the mouth and throat (don’t swallow).
When a cell becomes infected with a virus, they can express cytokines called interferons that can help the intrinsic defense of themselves and neighboring cells against viruses. See this Ninja Nerd Science video for a clear explanation from about 3:00 to 7:20 minutes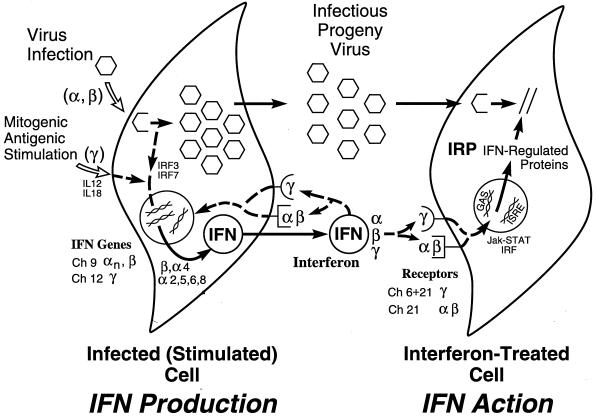
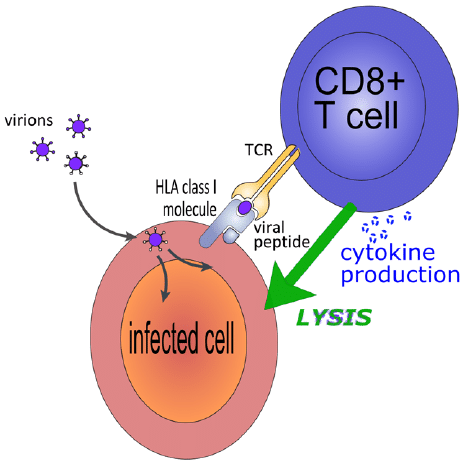
Once a cell becomes infected, it can also call upon a killer T-cell (CD8) to come and quickly kill it before it can continue to make and therefore spread more virions. This process of presenting a foreign viral protein (aka antigen) with its MHC-I or self-identifying receptor is illustrated in the following cartoon:
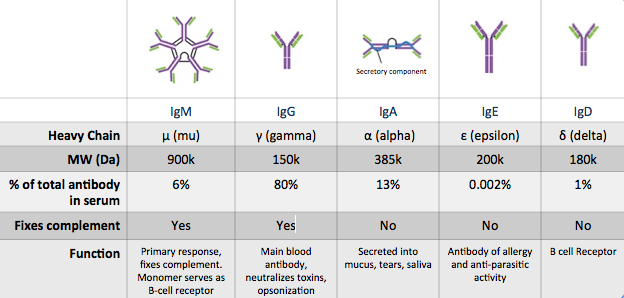
The basis of passive (maternal-fetal and breast milk) and adaptive (host-generated) immunity is based upon antibodies, which are specialized proteins meant to recognize epitopes (regions) of the dangerous proteins. We would prefer antibodies be directed towards proteins on the surface of the viruses but the process of destroying the viruses also creates antibodies to hidden and encapsulated proteins inside as well. A good example is that vaccines for Hepatitis B and HPV (the virus that causes genital cancers) are comprised of the surface proteins unique to those viruses so that the adaptive immune system can create specific antibodies to quickly clear them from the blood before they infect too many cells.
Because of the nearly infinite combinations of surface antigens that could be recognized, the immune system has to do two things well: it needs to REMEMBER the real threats that it has faced and it must be able to TOLERATE the body’s own cells so as not to trigger autoimmunity. The way it remembers is by having memory cells that have a specific ability to react to the threat if it ever presents itself; that is the basis of how we cure ourselves of new, repeated, and potential threats (in the case of vaccination). The way that the body learns to tolerate itself comes from the way T-cells are trained in the thymus. T-cells that are trained first must be positively selected for their ability to recognize the self-identity fingerprints known as MHC-I (the “us” factor) and MHC-II which are secret handshake fingerprints that allow for immune cells to communicate about new threats. Then they must be negatively selected and killed if they are too aggressive towards host cells. Finally, the naive T-cells leave the thymus, having been specialized to be CD4 (helpers) or CD8 (killers). They will be “naive” until they are needed to conduct an adaptive immune response to a new threat. Watch this wonderful Ninja Nerd Science video to learn more.
If a foreign infection creates enough of a new protein to trigger the host adaptive immune response either as a primary infection or as a repeat (anamnestic “didn’t forget”) response, then you get what is called clonal expansion (which is massive replication of a single clone with the enemy antigen’s identity) as well as even better refinement of antibodies in a process that occurs in those swollen lymph nodes that is known as somatic hypermutation. In other words there is purposeful improvement in the ability of the antibody-producing B-cells to attack the foreign antigens. 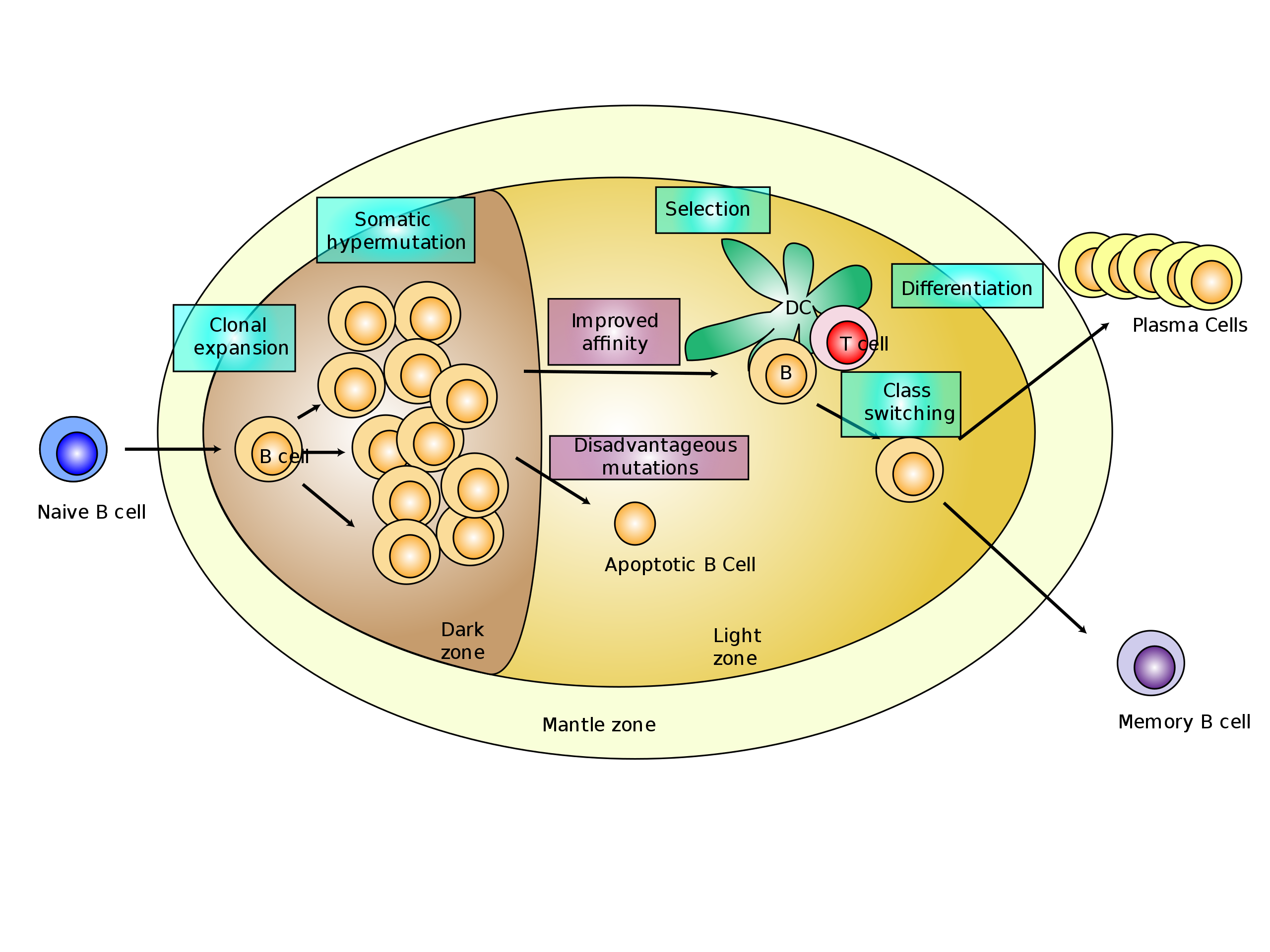
Since you may have a lot of spare time on your hands, I recommend this 14-minute video by the Ninja Nerd Science channel. It takes an incredibly complex subject and makes it very clear. If you really want to go deeper, watch this even more detailed 41-minute video on the adaptive immune system.
What is illustrated above is that process of your amazing ability to overwhelm foreign invaders using a combination of memory, adaptation, and exponential warfare against both new, old, and induced threats (as in the case of vaccination).
Okay…now that you understand a little about antibodies let’s just revisit two concepts. As I mentioned in blog 3, death from Covid-19 or any respiratory illness is more about the proverbial camel’s osteoporosis than the straw that broke its back (viruses). The bigger problem in all diseases, including infectious ones, is the depletion and degradation of our stem cells that comes with aging. In other words, immune senescence, probably from hematopoetic stem cell depletion due to telomere attrition and chronic herpesvirus infections, causes us to lack the numbers and flexibility of naive T-cells needed to respond to new threats and even older ones. The quality of immune response to viruses and cancers requires a reserve of naive but trained T-cells that come from naive and undifferentiated blood cell producing stem cells. Perhaps that is why telomerase activators anecdotally seem to help my patients fight of colds and flus and also why they improve antiviral function in HIV infected T-cells.
The second important concept is that we need a crystal clear understanding of what we are testing for in order to weigh the information that testing provides. There are three general types of tests we can do on patients: 1) PCR for RNA sequences specific to our virus that will test for the presence of the virus 2) serological assays to test for the presence of antibodies specific to our viral infectious response, and 3) viral load assays which are standardized estimates of the number of viral particles used to track the severity of chronic viral infections such as HepB and HIV. This is not available for less endemic viral infections.
Before we embark upon available tests, we need to define some basic biostatistical jargon. These terms assume that absolute truth can be known which is dubious, but as with the SIR epidemiolgical modeling discussed in the last blog, it is the best that we can do. A good start would be to look at the 2×2 grid for disease (aka the “confusion matrix” in machine learning. If you want to read about my opinions on why all AI is dangerous, read this blog.)
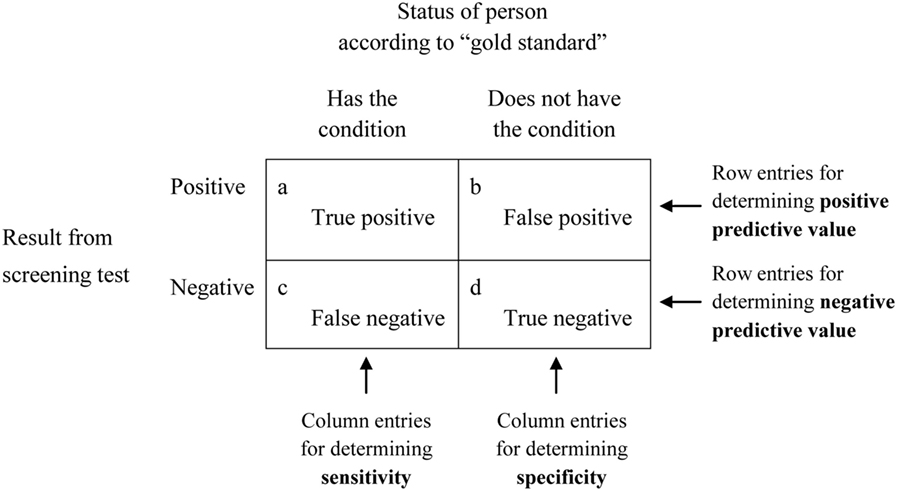
Ideally, we want tests with perfect predictive values but because of contamination, technical error, inconsistent reagents such as antibodies that are not exactly the same and tests that have cross-reactivity (act the same even if not perfectly identical), we have to a few of these terms. There are many more that derive from them.
The Sensitivity is the ability of a positive test to catch all the positive so it is TP/TP+FN (those the test missed). If you were testing for HIV in donated blood, you would want a very high sensitivity.
The Positive Predictive Value is the ratio of actual positives to all positives or TP/TP+FP (actual negatives).
The Specificity is the ability of a negative test to catch all the negatives so it is TN/TN+FP (those falsely positive).
The Negative Predictive Value is the ratio of actual negatives to all negatives or TN/TN+FN (actual positives)
Let me be very clear on this point, there are no perfect tests. By refinement in techniques and repeat testing, you can lower errors but this is not perfect and never will be…hence the limitations of scientific epistemiology that I referenced in the previous blog about epidemic modeling.
Let me explain as plainly as I can the types of testing that are available. You cannot see the virions unless you were to create a special probes and do tissue biopsies followed by electron microscopy. You cannot grow it in culture unless you use human tracheal culture, which is not a common technique. What you can do is 1) test for the RNA sequences with PCR and 2) infer that an immuno-competent person may was exposed from the serology (study of the serum antibodies).
PCR testing for viral RNA
Using the exact sequence of a string of nucleotides, the polymerase chain reaction technique is a highly sensitive and specific method of finding an exact sequence. Watch this 3-minute video to understand it.
PCR can only test for the presence of viral RNA which we assume correlates well with both active infection and infectiousness. Test kits use these standardized defined sequences of DNA primers of 18-24 nucleotides long that are going to match with regions in the CoV-WIV-1 (aka SARS-CoV-2) RNA genome if present. These were selected from the nucleocapsid proteins and are standardized by the WHO. I don’t know (but I hope) they knew what they were doing when they selected those regions as there can be mutations and we would expect conservation in sequence if there is conservation in function (i.e. the older coronaviruses might read very similar in sequencing.)
If the regions were the same across coronaviruses, then we would be testing for this and all previous endemic strains such as 229E, OC43, and NL63 and answering a very different question about what we used to think of as “a common cold” virus that occasionally becomes a flu-like illness and pneumonia in the immunocompromised.
If you thought the SIR epidemic modeling was a case of GIGO “garbage in-garbage out” then get ready for the really scary and depressing news. When it comes to testing for “immunity” via antibodies there are multiple problems. First, as we mentioned, the monoclonal antibodies are not always the same – there is a process of perfection and selection that takes place in the secondary lymph tissues like the nodes and spleen. So there isn’t just one key to fit the lock. If you don’t believe me, look at the variability in the types of commercially-available antibodies and proteins from just one company that match the current strain of SARS-CoV-2.
SEROLOGY
There are three types of testing for patient antibodies.
- RDT (rapid diagnostic test) – takes minutes and only tells you presence or absence.
- ELISA, which takes hours but can quantify the presence of specific antibodies (see video below).
- Neutralization Assay, which takes days but uses tissue culture to quantify how effective the patient’s antibodies are in a test tube at slowing a controlled amount of viral spread.
Here is a website showing some of the worldwide companies with serological tests for Covid-19. Note the alleged sensitivities and specificities although there is no true “gold standard” at all.
In this 2005 paper looking at 11 SARS patients, they found that there was cross reactive, non-specific antibodies that increased after infection. In other words, we assume they were battling SARS but the antibodies also rose for the run-of-the-mill CoV-229E (5 patients), and CoV-OC43 (10 patients).
If you made it this far, you may now intuitively understand the problem with testing. Since the immune system generates antibodies to many viral proteins and since the viruses are best attacked by surface proteins that are similar among cousins, we could be benefiting from partially effective immunity from previous bouts with the cold. In other words, the reason 40 of 60 recent asymptomatic blood donors in Castiglione d’adda (Lombardy) were seropositive were that the either the isolation didn’t prevent the majority of the herd from being infected (so the curve flattened because of depletion of susceptibles) and/or there is immunity to other coronaviruses that was being detected.
In a 2008 US study of 196 adults by Johns Hopkins, they found “The proportion of seropositive adults for each coronavirus was as follows: 229E, 91.3%; HKU1, 59.2%; NL63, 91.8%; and OC43, 90.8%“.
This may mean that serological testing will be misunderstood and misused for a variety of reasons, but mainly for profit and to further vaccine and public health surveillance. If you’re not concerned then I leave you with the disclaimer from one of the serology companies, United Biomedical: “Positive results may be due to past or present infection with non-SARS-CoV-2 coronavirus strains, such as coronavirus HKU1, NL63, OC43, or 229E”
So if you made it this far, you now know that the common cold strains of coronavirus may be conflated into the current Covid-19 statistics unless the PCR probes were absolutely unique to CoV-WIV-1. You know that previous memory B and T-cells are present in most of us from our many lifelong bouts with coronaviruses and confer some kind of cross-reactive immunity. You know that having a burned out immune system is deadly. And you might suspect that a vaccine is probably not as good as natural immunity in a young host and may confer unknown risks.
BONUS CONTENT – there are many treatments!
I leave you with one final Ninja Nerd Science Video on Covid-19 describing treatments and their mechanisms. This man has a real talent for explaining and you should might considering paying him as I did. He would have saved me a lot of effort if these had been available during medical school!
Add to that the publishing of in vitro results from Ivernectine and we have the makings of some pretty affordable and evidence-based ways of mitigating disease without waiting for a costly vaccine that could have poor efficacy, unknown risks, and high health care costs. People are so smart and resourceful when they are not paralyzed by fear of the unknown.
Keep on learning and please don’t be too quick to accept that we should acquiesce to a global 10% tithe to pay for a one-world pandemic authority, nor ankle tracking bracelets for Covid-19 contacts who refuse to self-quarantine, nor forced separation of families as per this WHO Dr. Ryan on March 30th (@49:27 …”Now, we need to go and look in families to find those people who may be sick and remove them and isolate them in a safe and dignified manner.”), nor citizens snitching on each other’s lock down violations for cash as LA mayor Garcetti is promoting.


5 thoughts on “Covid-19: Immunity and Testing”
Absolutely brilliant series of coverage on the current issue, thank you so so much Dr Ed we need more doctors like you in the world! Have you red a peer reviewed articled written by Dr Robert Young ? The Dismantling of the Viral Theory, Journal of Infectious Diseases and Therapy, Volume 6, DOI: 10.4172/2332-0877-C7-055 It worth your time to look the subject matter in hand from a different perspective. Much Love
A screening test may exhibit the shortcoming that the associated epidemiological model appears to the maker of a public policy on combating an epidemic to provide him or her with information about the outcomes of the events of the future without actually doing so. This can happen because a model makes an argument and this argument is not necessarily a logical one. An argument that is “logical” satisfies the law of identity, the law of the excluded middle and the law of non-contradiction. These are the “three classical laws of thought” of Aristotle.
An illogical argument can be and sometimes is dressed up to look like a logical argument through a misleading use of language by this argument. One of the ways in which this can happen is for a “projection” from a model to be mistaken for a “prediction” from this model because the phonemes and order of these phonemes of the two words make them easy to mistake for one another. Journalists and politicians are among the people who are prone to using these two terms synonymously but “projections” provide no scientific support for a public policy while “predictions” do. Case histories are presented in the peer-reviewed scientific literature in which politicians and journalists have mistaken “projections” for “projections” and this has led the politicians to make projections the bases for public policies though it is predictions that are required for this purpose.
A requirement for predictions to be made by a model is for random sampling to be conducted. Random sampling is not, however, conducted in the design of the study of the COVID-19 phenomenon that has thus far been conducted by epidemiologists under the Trump administration. In the daily briefing by the COVID-19 task force, Drs. Birx and Fauci correctly use the term “projections” in reference the outputs from the models that they use in advising the Trump administration on policy but fail to make clear to the journalists, politicians and ordinary citizens in the audience that these projections do not provide a scientific basis for the policy on COVID-19 that has been the result of their advice to the Trump administration. Contrary to what we are led to believe by them, for a study to be double blind and placebo controlled is not required for a public policy to have scientific backing. Random sampling is required but thus far not conducted.
More great info and wisdom!
Thank you for another great and thoughtful blog, but what do we do now? We’ve taken the most extreme measures possible to protect the weakest among us. We shut down our entire economy and changed our lives to flatten a curve. We carried Bambi across the minefield even though, as Dr. Park pointed out, Bambi probably couldn’t have destroyed the group. (Not that I mind, I would have proudly carried Bambi for no other reason but to save Bambi!) We can and should pat ourselves on the back for saving some lives, but nothing else has changed. If we continue life as it were before, the weakest among us will still die. There is no vaccine or cure. Now what? Continue extreme measures indefinitely? In the movie version, the hero would quickly develop a cure to save the day. I hope that will be our real-life ending here. It could happen! There are at least a couple of companies doing clinical trials using exosomes to treat COVID-19. Check them out here:
https://clinicaltrials.gov/ct2/show/NCT04276987?term=Exosomes&cond=COVID&draw=2&rank=1
https://www.thecurealliance.org/tag/covid-19/
Tanzania recently test pawpaw fruit and a goat. The tests came back positive. There is increasing evidence that these tests are flawed and/or contaminated. This whole event stinks to high heaven.