
Well it seems that my first five blogs were not the end of our Covid-19 discussions after all.
In my first five posts about COVID-19, I attempted to explain 5 things:
- Public health context of reducing spread: hand washing, fomites, and quarantine
- The emergence of an apocalyptic death cult. People harbor religious beliefs about COVID-19
- The greater scale of aging as a threat and how it contributes to all-cause mortality
- Coronavirus biology: origins, testing, and therapeutics
- How inflammation produces ARDS, the final common pathway for death from flu-like illnesses.
This sixth blog will explain epidemic modeling and the seventh will address serology and vaccines (or antibody testing for immunity). If there is an eighth, it might venture into the incredibly vexing area of biostatistics than delves into sensitivity, specificity, and predictive value. Take home point: I highly recommend watching the two embedded videos about modeling and coronaviruses below.
In the current situation, we are besieged by lies, damned lies, and statistics. A lie is when someone tells you they know what is going to happen based on math or their expertise; they do not because there are too many unknowns. A damned lie is when CBS misrepresents a picture of Italian hospital as a NYC hospital. And statistics (or epidemic modeling) is the realm that we will explore in this blog.
I supposed you could call this a blog and the next one about serology a no-holds-barred look at scientific epistemiology, or the study of knowledge itself; if you prefer, it can be thought of as a tour of the proverbial “sausage factory.” I will cut to the chase by saying that everything in the models of epidemiology is potentially flawed yet it is the best way of conceptualizing epidemics that we have. Allow me to explain.
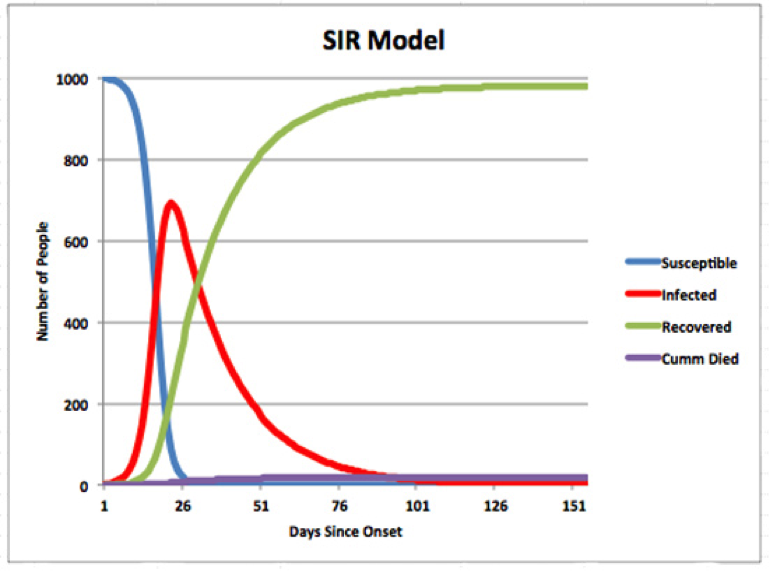
The standard SIR (susceptible, infected, resolved) model is where we get the exponentially growing and then exponentially declining curve that people wish to flatten with public health measures. A casual look at the three curves reveals several features of the model. As people go from susceptible to infected, there is exponential growth. As people transition out of infected to resolved (“cured” or deceased), then there is exponential decline in the infected curve. Towards the end of the epidemic there are no more susceptibles and the epidemic will never kill everyone (as some fear).
This 6-minute video is the best one I could find on the SIR model (N.B. he misspoke at 2:25 when he said R0 (r -naught or number of people one person will infect in the model) decreases with increasing duration of infectiousness; it actually increases))
For those us us who are critical thinkers, we might question the categories of this model. Firstly, we cannot assume that everyone is susceptible as there may be some partial immunity from previous common strains of coronaviruses such as CoV-229E, CoV-OC43, and CoV-NL63. In this study of CoV-SARS patients, the authors found that the “novel” 2003 CoV-SARS-1 would also stimulate antibodies to the older endemic versions proving there is cross-reactivity.
In other words, the numbers of S(susceptibles) may be lower and the R(resolved) might be higher if there is some partial immunity already in the herd, placing you somewhere else on the curve of an entirely different shape and magnitude. It is incorrect for anyone to suggest the behavior of the epidemic is not mitigated by previous exposures to coronaviruses because no one knows what the cross-reactivity is; perhaps the reasons there are so many asymptomatic young carriers is precisely because of partial immune anamnestic responses (the body recognizes the similarity of the surface antigens and makes usable antibodies). I have not heard from anyone suggesting that the actual surface antigens or epitopes of any of the coronaviruses are substantively different although I am open to seeing proof of that even though it contradicts logic. The main differences are in the proteins that are coded for by the RNA inside which could account for significant gain-of-function.
See my 7th COVID-19 blog (to follow) for further explanation on how antibodies work and are detected. The doctor below gives a very clear summary of coronaviruses, including the SARS and MERS variants and it was recorded before the current COVID-19 situation, rendering it less inclined to be skewed by the exceptionalism that rules the day.
Another problem is that just because a person is resolved, that doesn’t mean they can’t be reinfected unless deceased. There is no absolute way that you can say a person, despite having a robust immune response, can’t be at risk of returning to the infected if they have repeated, high level exposures, such as health care workers on the front line. Another problem of the SIR model is that populations are extremely heterogeneous. Young people with SARS-CoV-2 aka CoV-WIV-1 may be infectious for longer periods and have lower mortality. That is important when trying to predict future spread because the constants in the differential equations are very heterogeneous among subgroups and render your predictions to be less robust.
I find it dubious that draconian policy decisions were based upon model predicting 2.2 million deaths in the US and 500,000 deaths in the UK have since been revised down to 20,000 in the UK. The number is currently 4,400 with the UK on lock down). Many on the political spectrum have been guilty of underestimating the impact while still early in the exponential growth phase, including myself, I confess. Even Mayor Bill DeBlasio was encouraging New Yorkers to go out an enjoy the city as late as March 11th.
When all is said and done, if the number of deaths in the US falls well below the modelers’ predictions, there will be little recrimination nor loss of credibility because of the widespread beliefs in the seriousness of the threat. We all believe in the validity of “the curve” but conclusions about the magnitude based on constants that are unknowable are debatable. Also debatable are what repercussions we, as a society, would be willing to give up to flatten what would eventually flatten itself by all epidemic models. To discuss that doesn’t make you a science denier; it makes you an level-headed and free-thinking adult.
While it is alarming to have people die simultaneously and unacceptable to have them die for logistical reasons, the fact of any epidemic is that they cannot, as many fear, cause death on a massive scale unless you tweak several variables. Firstly, the case-fatality rate has to be higher but as the doctor above explained, when you have higher virulence as with CoV-SARS in 2003 (10% deaths) and the recurring MERS (35% deaths), the ability to spread among the general healthy public is limited. Remember these are case-fatality rates, not rates of all people who were exposed or infected since those population studies were never done. Now that we have corona awareness, we have novel data based on mass disease prevalence instead of just people with symptoms, that is yielding mortality rates of <1%.
It is precisely BECAUSE many young people are totally or relatively asymptomatic for long periods of time that this epidemic can spread efficiently. Secondly, the many antiviral and mitigating therapies that are being used can also mitigate the rate of transition from infected to resolved/practically immune.
In this recent paper by French epidemiologist comparing previous coronavirus infections and the current Covid-19 situation, Roussel et al show the mortality from this strain of coronavirus is not statistically different from previous strains that all of us have encountered in the past. I know that is hard to believe but that is what the data suggests. Look at the cases of Italy and Iran compared with other countries and you will have to question whether every nation is just “x-weeks from becoming the next Italy” as the media always warns us.
The fact is that when people every year die of “flu-like illness” no one ever used to bother looking for coronaviruses until now. It is only because we are looking for it that we find it; that is the very definition of “confirmation bias”. A multitude of viruses and other pathogens exist when people are hospitalized with pneumonia (sadly some are acquired BECAUSE of hospital or nosocomial infection) and the attribution to the “novel” Covid-19 is a major case of confirmation bias. In the current climate, if you are in the end stage of cancer and happen to get a positive CoV-WIV-1 test (even a false-positive), then you might be be classified as a victim of Covid-19.
Read this article by Dr. Iannidis who explains that absent the presumptive criminal, the number of flu-like deaths this season wouldn’t seem unremarkable given the annual totals. For example, the 2017-18 season was estimated to have taken the lives of nearly 80,000 Americans. For all we know (because we didn’t do the testing), a significant portion of those were triggered by the old coronaviruses such as 229E, OC43, and NL63 but we simply weren’t looking for them!
This “novel” Covid-19 appears to be much more similar in its behavior to those old endemic ones that we have faced and not at all similar to CoV-SARS and MERS which are MUCH more lethal but don’t spread as efficiently enough to create the disease prevalence and deaths of the current Covid-19 spread. Secondly, we never used to check for other coronaviruses when people die of ARDS from “flu-like illness” so they very well might have been a significant contributor in the past with several studies suggesting that if you got an old coronavirus, you had a 9 to 20% chance of dying if you made it to the hospital (because you were self-selected for co-morbidity and immune incompetence).
So, now that everyone is terrified of coronviruses and since I will fully concede that many of the high death tolls in past years may have been attributable to them, do we change our policies to reflect the new fear? It certainly seems we are headed that way.
Despite the fact that we survived year after year of coronaviruses and all the other pathogens creating epidemics and threatening us, it appears that the public policy will be generated based on models and heightened fear over coronaviruses.
We close with the case of Sweden which unlike nearly every other nation decided not to shut down everything and enact more limited measures like spacing people out at sporting events and limiting gatherings to 50 people. The public health experts there made a different risk assessment and concluded that the rest of the world was experimenting with reckless policies. Granted, Sweden has different population density than NYC but compared with neighboring Norway, their cases and are similar although 2-5X higher in the accumulated deaths (282 for 5,466 cases as of April 2nd). Unlike here in the US, Sweden report the ages and health conditions of all cases and they decided not to close schools, sports, and businesses. Despite the valuable “A-B test” in real time of Sweden, they may soon buckle to pressure to enact more extreme policies such as have taken hold in the rest of the world.
I have taken a lot of criticism from people suggesting there is blood on my hands since my second COVID-19 blog. Not one of them actually bothers to troll the media outlets, the Colin Powell’s, Robert Mueller’s, and George Bushes of the world who actually lied us into millions of dead people based on weapons of mass destruction. These zealots hold three articles of faith as I mentioned in blog 2: 1) this is novel, 2) this is deadlier, and 3) anything is worth flattening the curve. As I explained in blog 4, the RNA sequencing doesn’t show that much newness versus bat/pangolin strains although there are some that claim a gain-of-function, especially binding to Angiotensin2 receptors, was engineered. Some of the other proteins may have been altered but that doesn’t show up in a simple RNA comparison.
As the data rolls in from all countries doing testing, it appears that the biological and epidemiological behavior is very similar to the old coronaviruses which were admittedly deadly for some people but never being tested for. The economic and social collapse, suspension of liberties, and breakdown of humanity under a pervasive regime of fear is something that would be hard to justify based on the number of lives saved to date. Yes, I know, people are dying and even some young people. But wait until the inner cities run out of hope before you assert that it “was worth it.” We all seem to accept citations for going to public parks, hotlines for reporting neighbors being outside of the house, location tracking via smart phones, ankle bracelets for Covid-19 patients, and emptying prisons for felons with health conditions…all over the shared delusion that this is something new and deadlier that would justify any actions.
When a modeler revises death tolls from 500,000 to 20,000 they are still be hailed as a heroes of public health rather than fear-mongering Joe McCarthys. It seems clear that most people, when faced with censure from the good citizens yearning to report their neighbors for being reckless, are literally willing to do accede to anything to be seen to be compliant with the general consensus.
Let’s close with a common meme on Facebook, which is a good metaphor for the cluster-love that we are living through. This donkey, many are claiming, is being carried during WWII through a minefield so that it doesn’t set off land mines to kill everyone.
According to Snopes and multiple sources, the donkey named “Bambi” was injured and being carried back to the veterinarian by a Polish soldier in the 1958 Algerian war. While the point is taken the image is not apropos to the moral of the story. Even if we accept the meme’s premise, would that justify having the soldiers walking around a minefield without mine detectors in a spread out fashion? The donkey would likely only get itself killed, right?…it couldn’t set off a magical cascade of landmine explosions, would it? The story just doesn’t check out if you stop and think about it.
Likewise, unreasonable ideas and predictions about the COVID-19 situation become gospel when believed widely and not considered deeply. This simple photographic parable reveals itself to be a lie just like the worst-case scenarios of epidemic modeling that we have been presented with. An equally valid and recursive moral of the story should be that when posting memes and parables from the internet, you should use common sense and a little due diligence before virtue signaling. I wonder what memes people will post when they start shooting desperate people for looting food in densely populated areas? Trillions for banks and corporations but not much for the working poor unless they are vectors for disease transmission….it makes me wonder who the real donkeys are. I want to leave you with two general rules for self-correction: if you have ever used the phrase “it’s settled science” then you might not have a deep understanding of the scientific method. Secondly, if you say “I trust the experts” then you are probably not considering expert opinions that don’t confirm your biases.
There is nothing in this blog that I know to be factually inaccurate and as in the case with previous blogs I mean to inform, not inflame. Still, some will surely police my tone or disparage me based on the perceived subtext. If you perceive me as “minimizing the threat” despite simply reporting facts, my question to you is “why are you maximizing the threat” that has yet to be manifested when there is always an exponential decline to an epidemic and the mortality seems to be in line with the older endemic versions of coronavirus that 99% of us have antibodies to? Regarding the curve-flattening, you have gotten everything that you wished for and some things are coming that you would not have wished for. Are you hoping for higher death tolls to vindicate your argument or hoping for efficacy of mitigating therapies such as antivirals and other therapies like the recently FDA-approved hydroxychloroquine? Whose side are you on, really? What is your end game here?


14 thoughts on “COVID-19: Lies, Damned lies, and Statistics”
Well thought out comentary.
Very interesting and informative! You never disappoint. Humble and wise. People need to be highly educated in many complex concepts like economics, public health, history and common sense data interpretation to have an informed opinion about this issue as well as many other important issues. Thanks for sharing your very informed perspective which will surely get critiqued by lesser minds once again.
Thanks for being a sane voice in these bizarre times!
OMG, Doc. I am pleased no end to hear your take on this draconian overreaction to what is really just another “ flu season.”
I’m in the “target group.” I do not, in any case, expect to be the cause of the enormous reduction in freedom to save my ass, at the cost of a possible worldwide recession which can cause unnecessary suffering for millions of innocents for years to come.
Nobody gets out of here alive.
I’ve been binge watching WW II docs.
Now that was a problem. This is a panic due to either rank opportunists or an inflated fear of death.
I don’t want to get this thing, of course, but c’mon.
Tnx for your postings.
Movie in our future 🙏😊🙏
Missing elements in the construction of the models that are used by Drs. Birx and Fauchi in advising Pres. Trump on policy decisions include random sampling and cross validation of predicted outcomes. Given that these elements are missing, a model does not provide a suitable basis for policy decisions.
Experts don’t have a crystal ball
Dear Dr Par, this is yet another EXCELLENT article offering Common Sense approach to the challenge all Humanity is now experiencing. I’m trying to connect the dots by comparison and reconciliation of different scientific evidence – this one in particular got me truly puzzled – so I want to share it with your community.
In the following presentation, Dr Andrew Kaufman M.D. is comparing covid-19 viruses to body natural exosomes, finding them indistinguishable: youtube.com/watch?v=Xr8Dy5mnYx8
Take-out message is: science tells us that covid-19 virus does not exist. What is found in sick patients are their body natural particles (exosomes)!
Yes I watched that. Practically speaking they are similar but I believe that is because the virus uses the endocytic mechanisms like gathering in multivesicular endosomes before being extruded. They are both 125 nm spheres with RNA but the exosomes have discrete messages not one long genome
Pingback: Covid-19: Immunity and Testing | Recharge Biomedical
I have only read this blog and not your other articles. Found this one very interesting. Problematic to me is that none of the public health benefit analysis provided has done a comparison of the marginal cost to the marginal benefit of the steps being imposed. In other words let’s say hypothetically the models say there will be 60000 COVID 19 fatalities with a lockdown thru August and 100000 without one. Next let’s assume the lockdown leads to 20M unemployed, an increase in school children not being fed, an increase in sickness and mortality in both latter groups, and medical services not being made available to the balance of the population which causes collateral morbidity. Let’s leave out mental health issues. Let’s leave out domestic violence, increased crime and suicides which may increase. Also set aside that some communities cannot practically socially distance so it will not work there. Next set aside those who will not comply regardless. Note these are possible factors just like the assumptions epidemiologist are making. Has anyone put pencil to paper and calculated the other side of the equation so a rationale comparative decision is being made? Are there any rational assessments of the full equation being made or are we policy making with a WAG.
Well said
Pingback: Covid-19: Cognitive Dissonance and Cognitive Bias | Recharge Biomedical
Pingback: COVID-X: Experts wrong again | Recharge Biomedical
Hi,
Did you ever comment about the veracity of the claims about wearing masks, the types, can they be worn repeatedly, does cleaning make them less reliable and are they any use versus true medical grade masks. WSJ had an article today about the corruption occurring in the medical supplies markets and a recently seized shipment of flawed masks by FEMA(total ~500K). I also read a snippet of a clinical trial regarding the effectiveness of masks and SARS-CoV, it wasn’t favorable.
I guess you can tell I’m not a big fan. Haven’t worn one at all and been out for 2 months everywhere. Yesterday I did wear one in the grocery store because they asked. I get to the check out aisle, women has cheap masks and gloves. She coughs multiple times, so (drops) are probably getting on my items and I’m bare handed touching the card reader, etc. I can only think the Fed decided we need to let the people know masks help only to keep calm them.
Your thoughts?
Thanks